

Abstract
Introduction. Ruxolitinib (RUX) is the only targeted therapy available for the treatment of myelofibrosis (MF)-related splenomegaly and symptoms. Significant clinical responses may be achieved in around 50% of patients (pts). However, half of responding pts lose the response over time.
Aims. To report the outcome of a large cohort of MF pts after RUX failure, in terms of disease status, treatment strategies and survival.
Methods. A clinical database was created in 23 European Hematology Centers including retrospective data of 537 MF pts treated with RUX from Jan 2011 to July 2018. Updated information at the date of July 15th 2018 was available in 442 pts who were included in the present analysis. Spleen and symptoms response (SR & SyR) to RUX were evaluated according to the 2013 IWG-MRT criteria. RUX-related toxicity and infections were graded according to the WHO scale. Overall (OS) was estimated from the date of RUX discontinuation to the date of death or last contact, using the Kaplan-Meyer method (log-rank test).
Results. After a median follow-up of 30.5 months (1.7-84.3), 214 out of 442 evaluable (48.4%) pts had discontinued RUX. 43 (20.1%) died while on therapy because of: MF progression (34.9%), infections (25.6%), heart disease (16.3%), second neoplasia (7%), hemorrhages (7%), other (9.2%).
The median follow-up after RUX discontinuation for the remaining 171 pts was 11.3 months (0.5-66.7). Causes of RUX discontinuation were: drug-related toxicity (28.6%), loss/lack of response (23.4%), MF progression (12.3%), acute leukemia (AL) (13.4%), allogeneic stem cell transplantation (ASCT) (11.1%), second solid neoplasia (4.1%), other unrelated causes (i.e. pts decision; 7.1%).
After stopping RUX, 68 pts received 1 line of therapy, 21 received 2 lines and 9 received >2 treatments; 73 pts did not receive any therapy. Treatments received after RUX discontinuation, alone or in combination, included hydroxyurea (HU) (n. 61, 62.2%), ASCT (n. 20, 20.4%), second-generation JAK2 inhibitors (momelotinib/fedratinib/pacritinib) (n. 11, 11.2%), splenectomy (n. 7, 7.1%), azacytidine/decitabine (n. 5, 5.1%), chemotherapy (n. 4, 4.1%), investigational agents (imetelstat/PRM151: n. 4), danazole (n. 4), erythropoietin-stimulating agents (ESA) (n. 4).
A total of 95 pts (55.6%) died after RUX discontinuation, because of: MF progression (30.5%), AL (25.4%), infections (14.7%), second neoplasia (9.5%), hemorrhages (4.2%), heart disease (4.2%), ASCT (4.2%), thrombosis (2.1%), other (5.2). Median survival time from RUX stop of the 171 evaluable pts was 22.6 mos (95% CI, 13.2-30.7).
Among baseline features, survival after discontinuation was significantly influenced by the dynamic international prognostic score (DIPSS) category (p<0.001), transfusion dependency (p<0.001) and driver mutation status (with triple-negative pts having the worst survival compared to JAK2V617F and CALR-mutated pts, p=0.01).
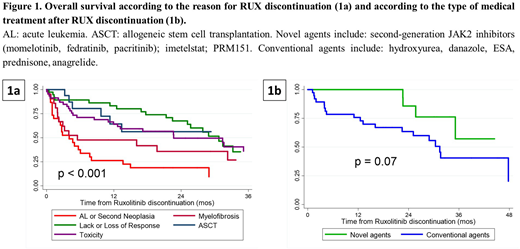
During therapy, 45 out of 153 (29.4%) and 123 out of 161 (76.4%) evaluable pts achieved a SR and a SyR at any time. Survival was not affected by the previous response to RUX at any time-point. Conversely, survival significantly differed according to the reason for stopping RUX, with pts discontinuing because of AL evolution/second solid neoplasia having the worst outcome (Figure 1a, p<0.001). In pts who discontinued RUX in chronic phase, the use of second generation TKIs and other investigational agents tended to prolong survival compared to the administration of conventional medical treatments (i.e. HU, danazole, ESA) (Figure 1b, p=0.07)
Discussion. After RUX failure, very limited therapeutic options are available and the prognosis of MF pts is dismal, particularly for those pts starting RUX with advanced stage disease (i.e. high DIPSS category and transfusion dependency). Also, disease evolution into AL and occurrence of a second solid neoplasia significantly reduced life expectancy. In chronic phase pts, survival probability may be improved by the use of medical therapies that are still in the experimental phase. Novel investigational agents are needed.
Palandri:Novartis: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Abruzzese:BMS: Consultancy; Ariad: Consultancy; Novartis: Consultancy; Pfizer: Consultancy. Vitolo:Roche: Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Gilead: Speakers Bureau; Takeda: Speakers Bureau; Sandoz: Speakers Bureau; Janssen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau. Aversa:Pfizer: Honoraria, Membership on an entity's Board of Directors or advisory committees; Basilea: Honoraria, Membership on an entity's Board of Directors or advisory committees; Merck: Honoraria; Astellas: Honoraria; Gilead: Honoraria, Membership on an entity's Board of Directors or advisory committees. Cuneo:Gilead: Other: advisory board, Speakers Bureau; Roche: Other: advisory board, Speakers Bureau; Abbvie: Other: advisory board, Speakers Bureau; janssen: Other: advisory board, Speakers Bureau. Foà:ROCHE: Other: ADVISORY BOARD, Speakers Bureau; AMGEN: Other: ADVISORY BOARD; JANSSEN: Other: ADVISORY BOARD, Speakers Bureau; GILEAD: Speakers Bureau; NOVARTIS: Speakers Bureau; CELTRION: Other: ADVISORY BOARD; ABBVIE: Other: ADVISORY BOARD, Speakers Bureau; INCYTE: Other: ADVISORY BOARD; CELGENE: Other: ADVISORY BOARD, Speakers Bureau. Di Raimondo:Celgene: Honoraria; Takeda: Honoraria, Research Funding. Cavo:Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Bristol-Myers Squibb: Honoraria, Membership on an entity's Board of Directors or advisory committees; GlaxoSmithKline: Honoraria, Membership on an entity's Board of Directors or advisory committees; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees; Adaptive Biotechnologies: Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees. Breccia:Pfizer: Honoraria; Incyte: Honoraria; BMS: Honoraria; Novartis: Honoraria. Palumbo:Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal